
Cartilage tears

The knee is described as being made up of three compartments. There is the medial and lateral, or inner and outer aspects, of the knee joint itself. And then there is the space between the kneecap and the rest of the knee, the so-called patellofemoral space.
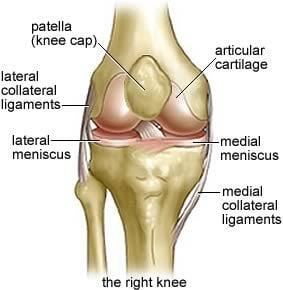
Each of the medial and lateral compartments of the knee contain a meniscus. This is made up of fibro cartilage. These cartilages allow the knee to move smoothly, and they play a role in stabilising the knee and aiding in control of rotation movement.
Both the cartilages also help to absorb compressive forces in the knee as body weight is transmitted through the legs. The cartilages act as shock absorbers to protect the lining of the knee joint.
The meniscus attach to surrounding ligaments and move with movement of the knee. The position of the cartilages change slightly as the knee is straightened and bent. The cartilages also move with rotation of the knee.
Cartilage tears are common. The most common age group for this is the 20 to 30-year-old age group. The inner or medial cartilage is more commonly torn in the lateral cartilage.
Cartilage injuries are more common in people who squat or kneel, such as floor layers. They commonly occur with a lot of kneeling or squatting and simultaneous twisting.
As we age, the cartilage becomes less supple and with osteoarthritis of the knee, degenerative tears in the cartilage are common. These may occur with minor trauma, or without trauma.
The cartilage may be damaged by itself, or damage may occur to any of the other structures of the knee, depending on the level and type of trauma. The articular surface or lining of the knee may be damaged and if this occurs, osteoarthritis of the knee can occur as a late complication.
If the force that causes the cartilage to tear is substantial, there may be damage to one of the other ligaments of the knee, such as the collateral ligaments or the cruciate ligaments.
Types of tears
Tears may be small or large, and tears may run horizontally or longitudinally. A “bucket handle” tear can occur, and part of the cartilage may become detached and move into other areas of the joint where it can cause locking.
Clinical features
Cartilage tear usually causes pain that is suddenly an onset, substantial pain, and is felt inside the knee - often on the side where the tear occurs.
Typically, the person who sustains a sudden cartilage tear is unable to continue with their activity.
A degenerative tear does not usually cause immediate severe pain, and the problem may develop gradually.
Cartilage tears can cause swelling of the joint, and can cause the joint to lock or not be able to move. Many patients complain of clicking; the clicking is often painful and often audible. Patients with cartilage tears can also complain of the knee feeling unstable.
Making a diagnosis
The history is the main feature that helps clarify a diagnosis. MRI scans are by and large reliable when diagnosing cartilage tears.
If a cartilage tear is suspected, the person should receive an urgent MRI scan so the problem can be managed quickly and efficiently.
Surgery is the most appropriate form of treatment for a cartilage tear. Orthopaedic referral should occur early.
Most patients have a good result from surgery. The most common operation is to trim the area where the cartilage is torn. Occasionally the tear can be repaired, and occasionally almost all of the cartilage or meniscus needs to be removed.
Osteoarthritis is common after meniscectomy. This is more of an issue with the lateral or outer meniscus and is more common with total rather than partial removal of the meniscus.
A cartilage injury and meniscectomy can also accelerate osteoarthritis in someone who is already experiencing an arthritic knee.
Key aspects of work injury management
People who sustain a cartilage tear are restricted in what they can do.
A cartilage tear can be managed quickly, or the process can be drawn out. Earlier management is associated with earlier return to work.
The benefits of early management are substantial, but require a coordinated approach that often does not occur.
What often happens
- Dave stumbled over a pallet 3 months ago.
- He attended the doctor the next day with his sore left knee after it became swollen overnight.
- His doctor recommends physio.
- Physio continues for 3 weeks.
- Appointment with Orthopedic Surgeon takes 2 weeks to obtain (if you are lucky).
- Orthopedic Surgeon recommends arthroscopy, takes insurer 5 weeks to obtain a medical report and accept the costs of surgery will be covered.
Dave’s surgery is completed 3 months after the injury. He has been working but has been significantly less productive. He’s also pretty frustrated at hanging around waiting for the next step.
Best practice approach
- The workplace understands Dave hurt his knee and that the knee is swollen, so it’s likely a significant injury.
- Dave is seen by a treating doctor.
- MRI arranged within one or two days with review by orthopedic surgeon within a few days.
- Liaise with insurer to have arthroscopy approved without delay.
Dave’s arthroscopy is completed by one week post injury. He is back at work on modified duties a week later, and back at his normal job within three weeks of the injury.